
Modeling Spanish anxiolytic consumption: Economic, demographic and behavioral influences
Abstract
Anxiolytics (AX) are the psychotropic drugs prescribed for the treatment of anxiety and insomnia for 2–4 weeks, for longer periods of consumption (>1 month) may lead to the development of tolerance or addiction. In fact, its prescription was 16% of the total pharmaceutical expenditure in Spain in 2007. This paper deals with the development of a mathematical model describing the dynamic of the addiction to AX for the case study of the Spanish region of Castellón. The reasons believed to cause the development of addicts to AX are the economic situation, the marriage termination and the social contact. The simulations performed to forecast the addicts rate for the period 2010–2014 showed an increase from 6% in 2010 to 14% in 2014 with a fluctuation of about 2% between the possible economic scenarios. Finally, the analysis of sensitivity of the rate of addicts to the fluctuation of the social contact parameters was performed, letting us estimate its impact on the pharmaceutical expenditure.
Keywords
Anxiolytics; Addiction; Pharmaceutical expenditure; Social contact; Marital termination; Economic scenario.
Authors
E. De la Poza
Departamento de Economía y Ciencias Sociales, Universitat Politècnica de València.
N. Guadalajara
Departamento de Economía y Ciencias Sociales, Universitat Politècnica de València.
L. Jódar
Instituto Universitario de Matemática Multidisciplinar, Universitat Politècnica de València.
P. Merello
Instituto Universitario de Matemática Multidisciplinar, Universitat Politècnica de València.
LINK: Artículo en www.sciencedirect.com
Abril 2013
1. Introduction
Of all psychotropic drugs (antidepressants, antipsychotics, anxiolytics (AX) and analgesics opioid group), the most prescribed medications are AX belonging to the group of benzodiazepines [1] N05B, code defined as the classification system Anatomical Therapeutic Chemical (ATC). The main causes of the prescription of AX by the general practitioners (GP) of Primary Health Care Centers (PHCC) are the presence of anxiety and/or insomnia [2, 3]. The causes of the emergence of these diseases may be the presence of chronic diseases [4], or social, economic and demographic variables [1].
In Spain, the consumption of AX has increased significantly since the 90s. In fact, in 2007, it represented the 16% of the total pharmaceutical expenditure. In 2009, 15.5% of Spanish population consumed AX in a regular basis and the public expenditure of it summed up over 200 million Euros.
These drugs are only suitable for short-term treatment (between 15–30 Defined Daily Doses (DDD) ≈ 1 month). However, several studies show that GP often prescribe treatments for longer, which increases the risk of patients developing tolerance and physical or psychological addiction [5]. The consequences of developing drug dependence may lead to brain damage resulting in poor concentration, reduced ability to react, memory loss, and accidents. It should seek alternative therapies to psychopharmacology, to reduce not only the economic cost, but also the social cost [6].
Also several studies have been developed in analyzing the ability of patients who have taken sedatives for over a year to reduce and eliminate their consumption [7, 8].
Recent studies show how the consumption of AX increases with the age of the patients; consumption is more common in women than in men [9], in singles, divorced or widowed than married [10] and in situation of unemployment [11], in general people who show lower levels of well-being. Also, the social contact could play an important role in all levels of consumption of AX, as occurring with other addictive behavior (nicotine, shopping, food) [12, 13]. Previous studies [12, 13] develop discrete mathematical models considering that social contact may spread from one person to another by the interaction of individuals [14, 15].
The aim of this paper is to develop a mathematical model to predict addictive behaviors to AX by social contact. For this purpose, the population of the study is grouped into three levels according to their level of AX consumption: incidental user, regular user and long-term user (those who have developed addiction). This will lead us to estimate the social effects, the pharmaceutical expenditure, and possible public health recommendations. The paper is organized as follows. Section 1 is an introduction; Section 2 develops the mathematical model and presents the hypotheses and sources of information considered; Section 3 shows the results obtained from different economical scenarios simulated. Finally, the main conclusions are shown in Section 4.
2. Method
2.1. Information sources
The study population in this work is made up of subjects who were registered as inhabitants in the Census of the province of Castellón in the Autonomous Community of Valencia (Spain) and also were registered in the Population-based Information System (SIP) in the province of Castellón in 2009 and 2010. The region of study was selected because of the implementation of the electronic prescription system (RELE system) at the end of 2008. Let us note that each inhabitant is provided a SIP number to be identified within the National Health System.
Information about the prescription of AX at PHCC in the province of Castellón in 2009 and 2010 was provided by the Regional Valencian Government’s General Pharmacy Management. Data was already codified according to the Organic Law 15/1999 on the Protection of Personal Data.
The two databases analyzed (one from 2009, the other from 2010) consisted of 597,844 rows and 591,804 rows, respectively and 5 columns embracing the code of each person, their gender, age, number and cost of DDD of AX prescribed.
2.2. Mathematical model and hypotheses
To build the mathematical model, the population is divided into three subpopulations according to the AX (number of DDD) prescribed by year [9]: A: long-term users (more than 180 DDD ≈ more than 6 months); R: regular users (31–180 DDD ≈ 2–6 months); I: incidental users (0–30 DDD ≈ 1 month). The subpopulation of incidental consumers (I) includes all people that have never consumed for the period considered or they have done just occasionally.
The total population (P) at any time n is expressed as follows:
Pn=In+Rn+An
The factors considered in the development of addiction to AX consumption were the economic scenario, the marriage termination (embracing marital dissolution through divorce, separation and annulment) and the social contact.
The dynamic of the population can be described by Fig. 1 and the following system of difference equations (n, time in years):
In+1−In=β(In+Rn+An)−diIn−αIn+γ1Rn+γ2An−μ1InAn−ψIn,
Rn+1−Rn=−drRn+αIn−αRn−γ1Rn+γ1An+μ1InAn−μ2RnAn+ψIn−ψRn,
An+1−An=−daAn+αRn−γ1An−γ2An+μ2RnAn+ψRn.
The model was built following the assumptions of previous socially contagious studies [12, 13]. The values of all parameters were estimated from different sources of information and hypothesis with the exception of the transit rates (μ1,μ2) that were adjusted by the model.
Fig. 1. Dynamic of the population.
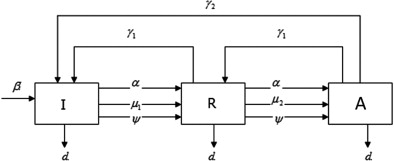
The parameters of the model are:
- β, birth rate of the population, where β=0.00107 of Castellón for 200916, according to INE (Spanish Institute of Statistics). We consider the birth rate forecasted by INE for the period 2011–2014.
- d
z
- , mortality rate by categories of AX consumption (z=i,r,a). We used INE information about the mortality rates by age intervals. We adjusted the mortality rate of each category of AX to their age proportion. Let di=0.024038,dr=0.0355799, da=0.0276696.16.
- γ
1
- , rate of recovery of addictive consumers to regular consumers or transit of regular consumers to incidental consumers through a therapy of discontinuation of AX. We estimated this parameter following studies
- ,
- and
- related to the discontinuation of AX prescription through interventions (letter, therapy, etc.) as γ
1
- =0.015. The recovery process is determined by the primary action of the GP who has to diagnose the patient’s addiction defining a therapy and second the patient who has to admit his illness.
- γ
2
- , rate of recovery of addictive consumers that become incidental consumers after therapy (change of medication) with other substances. We assumed that addicts aged less than 50 years old could become incidental consumers if other medication substances different from AX replaces their AX prescription. The parameter is estimated as follows: we know from our database that the proportion of addicts aged less than 50 years old over the total number of addicts (26.66%), while we assume the proportion of addicts younger than 50 years old whose medication changes (3%). Due to the average rate of success of the new medication (55%) [
- ], this way, γ
2
- =0.2666×0.03×0.55=0.0043989
- α, rate of unemployed people that consume AX, where α=0.0273 in 2010. This rate is considered independently of the level of consumption. We assume that the 20% of unemployed people in Castellón (23.96% (fourth trimester 2010)) older than 35 years old (57% population of Castellón)16 increases the consumption of AX, becoming a regular or long-term consumer. (α=0.2×0.2396×0.57.)
- ψ, rate of marriage termination (divorce, separation, annulment). As a result, they develop stress and mental disorders [
- ], becoming regular users and addictive users over time [
- ]. It was considered constant for all categories of consumption. ψ=0.000355. We estimated the following: we assume that the 15% of the total employed people of Castellón in 2009 (76.04% of population), who terminated their marriage (3.1175%; average rate in the Valencian Community for the period 2006–200916) transit to a higher level of AX consumption [
- ]. This way, ψ=0.7604×0.15×0.031175=0.000355.
The parameter «social contact» explains the social influence the long-term user of AX has, modifying others’ behavior. The development is just the consequence of the interaction between individuals. The effectiveness of the social propagation is based on the word of mouth communication of the AX long-term user (A). We assume that only long-term AX users (A) are capable to influence others’ behavior. So, the social propagation rates estimate the transfer rates between subpopulations as consequence of the social contact of incidental (I) or regular users (R) with long-term users (A).
- μ
1
- , transit rate of incidental consumers to regular consumers due to «social contact» with addicts. (Incidental user → regular user.)
- μ
2
- , transit rate of regular users to long-term consumers due to «social contact» with addicts. (Regular user → addicts.) We consider that the social contact influence is higher in regular consumers than in incidental ones, μ
1
- < μ
2
- . It is assumed that no consumer transits from incidental to addict consumer.
The social contact parameters μ1 and μ2 are adjusted using the databases previously described and implementing, as in 12 and 13, the Nelder–Mead algorithm for finding a local minimum of a function of several variables, applying Mathematical software. Once the parameters were estimated, we forecast the consumption of AX assuming different economic scenarios for next four years (2011–2014), considering this period of time appropriate due to the available sources of information of the parameters trying to minimize the error of the estimations.
2.3. Economic scenarios
Different simulations are developed considering that the value of α evolves during the next four years assuming different economic scenarios [20].
- Scenario L: the economic crisis will remain for at least 5 years (long-term recovery).
- Scenario V: the economic recovery will happen in one year and a half (short-term recovery).
- Scenario: at first, there will be a little relapse, in the second year the economic situation will suffer a recovery and then will remain constant.
- International Monetary Fund (IMF) Scenario [
- ]: a strong recovery for the first year, and then a constant recovery (unemployment rate decreases at 1% per year) for next 4 years.
- Optimistic Scenario: the unemployment rate decreases over time.
With the aim of analyzing exclusively the social contact effect, we simulate different values for μ1,μ2 between the interval [1/2μ,3/2μ], while the rest of the parameters remain constant.
3. Results
The first row of Table 1 shows the composition of the population by categories of AX consumers for 2010. The 88% of total population were incidental consumers in 2010, while the long-term consumers resulted to be slightly higher (6.22%) than the regular consumer category (5.42%). The average pharmaceutical expenditure of each patient’s category was 1 Euro for the case of incidental consumers, 100 Euros for the regular consumer category and 643.66 Euros for a long-term consumer in 2010.
Table 1. Forecast of consumers of AX by subpopulation and economic scenario.
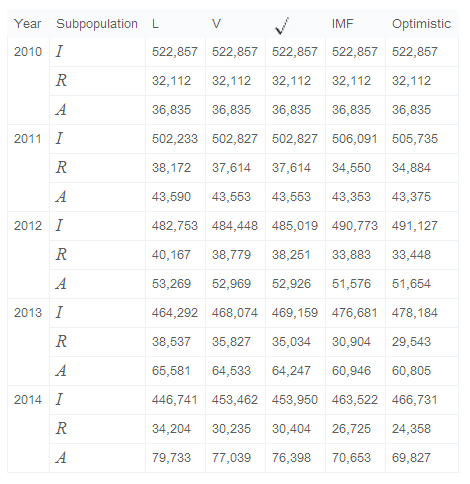
The value of the parameters μ1 and μ2 were obtained using Nelder–Mead algorithm: μ1=6.598×10−21 and μ2=6.365×10−6. The results obtained show how the rate of transit of incidental to regular consumers due to their «social contact» is almost null.
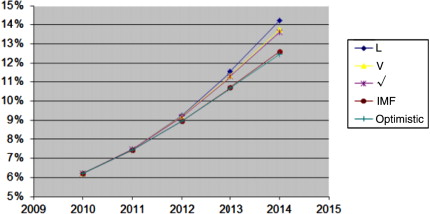
The prediction shows an increase in the number of long-term consumers of AX for all economic scenarios, (Table 1). In fact, the mathematical model forecasts about 13%–14% of the total population of Castellón, which will be addicted to the consumption of AX in 2014, while this subpopulation was about 6.22% in 2010. The results between economic scenarios fluctuate about 2% in 2014. Fig. 2 shows the differences between economic scenarios for long-term consumers.
Fig. 2. Development of the percentage of long-term consumers of AX by economic scenarios.
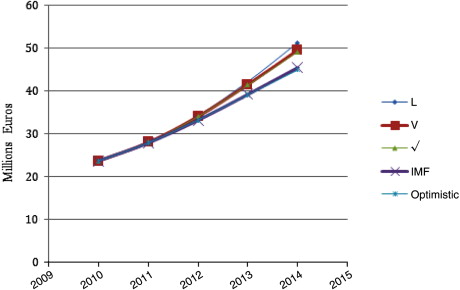
Then, we estimated the public healthcare expenditure derived from the prescription of AX for the next four years and different economic scenarios considering the average expenditure for each category is constant for each year and equivalent to the 2010 cost. This implies that we assume there is no inflation effect and also there are no healthcare policies to reduce the Pharmacological Budget (i.e. Generics use, co-payment, etc.). Fig. 3 shows the increasing trend of the AX expenditure which will be doubled in four years, since data shows an increase from about 23 million Euros to over 51 million Euros in 2014 in the worst possible scenario (Scenario L) or close to 45 million Euros in the best alternative (Optimistic Scenario).
Fig. 3. Increasing trend of the AX expenditure.
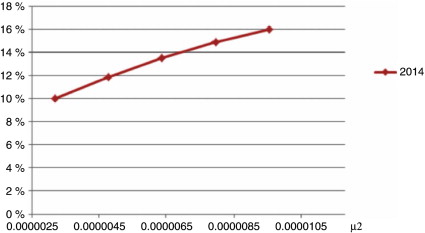
Finally, we analyze the sensitivity of the percentage of addicts to the fluctuation of the social contact parameters μ1,μ2 between the interval [1/2μ,3/2μ]. The simulations were made assuming all parameters are constant and the rate of unemployment was estimated as the average rate of unemployment of all possible economic scenarios considered for each year (Scenario L, V, , IMF, Optimistic). Since there are two social contact parameters μ1, μ2 with different fitting values, we will simulate each parameter μ1, μ2 considering the other one remains constant.
The sensitivity of the percentage of addicts to the oscillation of μ1, was almost null, since the subpopulation of addicts practically remain constant for all possible economic situation. However, as Fig. 4 shows, a decrease or increase of the parameter μ2 of 50%, produces an oscillation from 10% to almost 16% of the AX addicts rate, respectively, what would mean in economic terms a public expenditure over 57 million Euros (3/2μ2), or 36 million Euros (μ2/2).
Fig. 4. Analysis of sensitivity of the number of addicts to the change of the parameter μ2.
4. Conclusions
The paper presents a prospective model to forecast the level of consumption of AX for the next four years (2011–2014) in the province of Castellón considering as main variables, that can influence the AX consumption, the social contact, the economic situation, and the marital termination.
The mathematical model lets us predict the future number of regular and addicts to AX, and as a result the volume of DDD prescribed and their public expenditure.
Considering the demographic, economic and cultural similarities between provinces, this can be applied to any Spanish province or the whole country. For the particular case of Castellón, the percentage of consumers will double from 2010 to 2014. As a consequence, the public expenditure of AX will increase for all possible economic scenarios, measured through the rate of unemployment.
The results obtained should be considered as a valuable source of information for Public Authorities in order to control and reduce the AX prescription by GP through different policies, mainly alternative therapies to the pharmacological ones since the results obtained show how the GPs’ prescribing patterns are not in accordance with recommended dosage and duration of AX treatment.
On the other hand, the social contact plays an important role in the development of addiction of AX as already shown in other studies 12 and 13. We have observed an important oscillation of the percentage of addicts when the social contact rate (μ2) fluctuates. This fact shows the relevance of the Public Authorities to educate the population about the effects of the addiction to AX in order to prevent the population in risk (low self-esteem) to become addicts.
Finally, as limitations of our study we could name the non-consideration of other variables that can influence the prescription of AX due to low esteem levels (physical disabilities or relatives pass away), due to their difficulty to be measured, and also the interaction between the variables of the model (i.e. effect of divorced people is considered as a static variable and not as a dynamic; the interaction between mortality rate and divorce, unemployment rate and mortality, or unemployment and birth).
Acknowledgment
The authors wish to thank the DGF of the Regional Valencian Ministry of Health for generously providing access to the databases required to conduct this work.
References
1. A. Bocquier, K. Bezzou, S. Nauleau, P. Verger. Dispensing of anxiolytics and hypnotics in southeastern France: demographic factors and determinants of geographic variations. Fundamental & Clinical Pharmacology, 22 (2008), pp. 323–333
PDF Full Text
2. C. Vedia, S. Bonet, C. Forcada, N. Parellada. Estudio de utilización de psicofármacos en atención primaria. Atención Primaria, 36 (5) (2005), pp. 239–247
3. S. Kisely, M. Linden, C. Bellantuono, G. Simon, J. Jones. Why are patients prescribed psychotropic drugs by general practitioners? Results of an international study. Psychological Medicine, 30 (2000), pp. 1217–1225
Abstract at PubMed
4. N. Guadalajara, I. Barrachina, E. De la Poza, D. Vivas, M. Caballer. Modelling the consumption of anxiolytics and its addictive behaviour. Mathematical and Computer Modelling, 54 (7–8) (2011), pp. 1626–1633
5. R. Van Hulten, A.B. Bakker, A.C. Hubert, G. Leufkens. Determinants of change in the intention to use benzodiazepines. Pharmacy World and Science, 23 (2) (2001), pp. 70–75
Overview at rug.nl
6. B.M. Verdel, P.C. Souverein, T.C.G. Egberts, T.P. van Staa, H.G.M. Leufkens, F. De Vries. Use of antidepressant drugs and risk of osteoporotic and non-osteoporotic fractures. Bone, 47 (3) (2010), pp. 604–609
Abstract at PubMed
7. A. Veronese, M. Garatti, A. Cipriani, C. Barbui. Benzodiazepine use in the real world of psychiatric practice:low-dose, long-term drug taking and low rates of treatment discontinuation. European Journal of Clinical Pharmacology, 63 (2007), pp. 867–873
Abstract at PubMed
8. S.E. McCabe, J.A. Cranford, B.T. West. Trends in prescription drug abuse and dependence, co-occurrence with other substance use disorders, and treatment utilization: results from two national surveys. Addictive Behaviors, 33 (10) (2008), pp. 1297–1305
Abstract at PubMed
9. R. Van Hulten, H.G. Leufkens, A. Bakker. Usage of benzodiazepines in a Dutch community: a 10-year follow up. Pharmacy World and Science, 20 (1998), pp. 78–82
Abstract at springer.com
10. L. Manthey, T. Van Veen, E.J. Giltay, J.E. Stoop, A.K. Neven, B.W.J.H. Penninx, F.G. Zitman. Correlates of (inappropriate) benzodiazepine use: the Netherlands Study of Depression and Anxiety (NESDA). British Journal of Clinical Pharmacology, 71 (2) (2011), pp. 263–272
Abstract at PubMed
11. A. Dragun, A. Russo, M. Rumboldt. Socioeconomic stress and drug consumption: unemployment as an adverse health factor in Croatia. Croatian Medical Journal, 47 (2006), pp. 685–692
Abstract at PubMed
12. I. García, L. Jódar, P. Merello, F.J. Santonja. A discrete mathematical model for addictive buying: predicting the affected population evolution. Mathematical and Computer Modelling, 54 (7–8) (2011), pp. 1634–1637
Full text at sciencedirect.com
13. F.J. Santonja, R. Villanueva, L. Jódar, G. González-Parra. Mathematical modelling of social obesity epidemic in the region of Valencia, Spain. Mathematical and Computer Modelling of Dynamical Systems, 16 (1) (2010), pp. 23–34
Abstract at tandfonline.com/
14. N.A. Christakis, J.H. Fowler. Connected: The Surprising Power of Our Social Networks and How they Shape Our Lives. Hachette Book Group (2009)
15. R.E. Emery, D. Sbarra, T. Grover. Divorce mediation: research and reflections. Family Court Review, 43 (2005), pp. 22–37
Abstract at wiley.com
16. Spanish Statistical Institute. Available at: http://www.ine.es
17. J.D. Morgan, D.J. Wright, H. Chrystyn. Pharmacoeconomic evaluation of a patient education letter aimed at reducing long-term prescribing of benzodiazepines. Pharmacy World and Science, 24 (6) (2002), pp. 231–235
Abstract at PubMed
18. J. Bobes, G. Rubio, A. Terá, G. Cervera, V. López-Gómez, I. Vilardaga, M. Pérez. Pregabalin for the discontinuation of long-term benzodiazepines use: an assessment of its effectiveness in daily clinical practice. European Psychiatry (2011)
Abstract at PubMed
19. R.D. Kocalevent, A. Hinz, E. Brähler, B.F. Klapp. Determinants of fatigue and stress. BMC Research Notes, 4 (2011) Art. no. 238
20. A. Trías, De la V a la L, el abecedario de la salida de la crisis (in Spanish).
21. International Monetary Fund, World economic and financial surveys, World economic outlook database.
http://www.imf.org/external/pubs/ft/weo/2011/01/weodata/index.aspx
Máster en Gestión Sanitaria Online 2023/2024

Información detallada del Máster:
Artículos completos en la web del CIEGS
Impact of population morbidity on health care costs in a health district.
Análisis de costes en el Área de Imagen Médica de grandes hospitales españoles.
Predictability of pharmaceutical spending in primary health services using Clinical Risk Groups.
Pharmaceutical cost management in an ambulatory setting using a risk adjustment tool.
Is Health Related Quality of Life (HRQoL) a valid indicator for health systems evaluation?
Atención a mujeres inmigrantes en un programa de mediación intercultural en salud.
Modeling Spanish anxiolytic consumption: Economic, demographic and behavioral influences.
Sistema de prescripción y dispensación electrónica en la Agencia Valenciana de Salud.
Incidencia y variabilidad de la incapacidad temporal por trastornos de ansiedad en la Comunidad Valenciana durante el 2009.
Costes y procesos hospitalarios en neurología. Estudio en un hospital de referencia.
Claves para motivar y fidelizar a los médicos especialistas.